Posted 21 April 2020
Today is biology/medicine today.
Having now completed the module on coronavirus that appeared yesterday in my on-going nutrient lecture course, what better way to consolidate the knowledge than to distill the key points!
I derive an explanation of the ‘cytokine storm’ you may have heard of and conclude the piece with some input on vaccines.
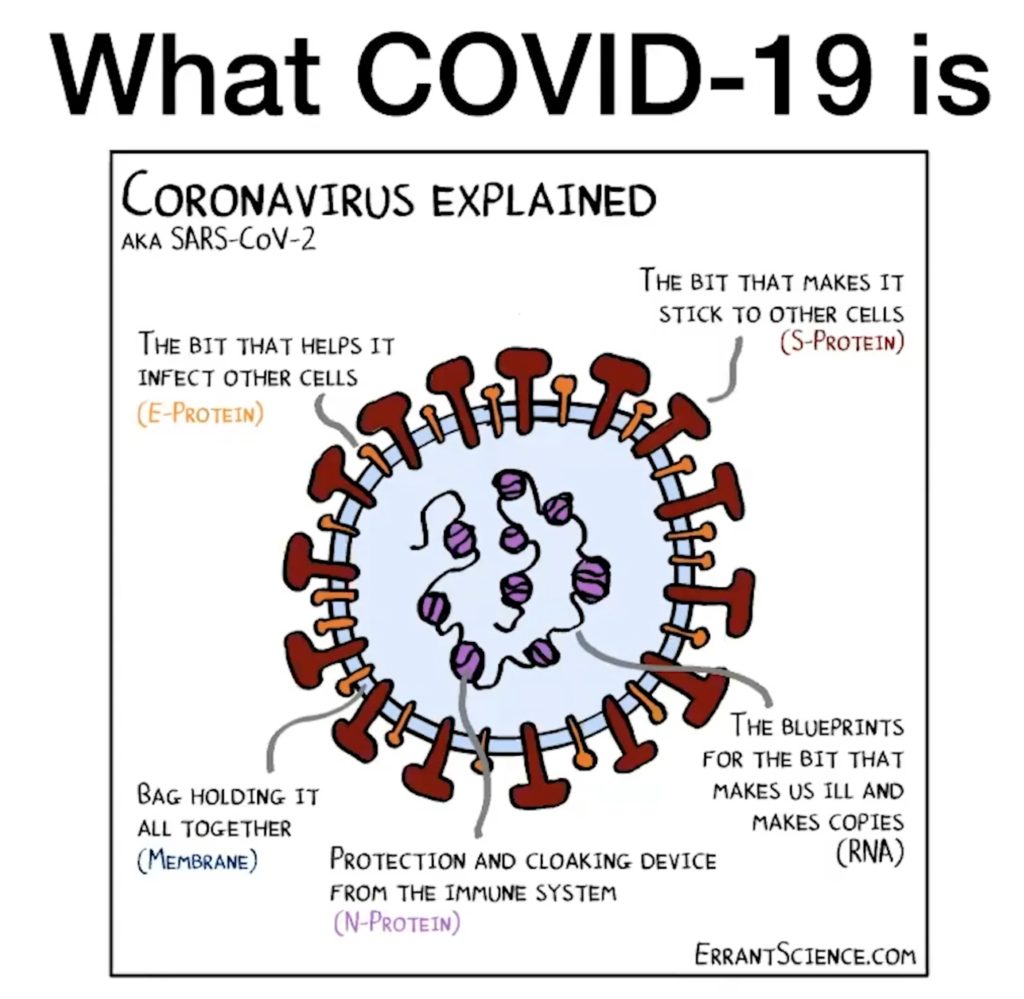
1. SARS Virus is an RNA virus. It comprises a strand of genetic material called ribonucleic acid (RNA) which is the blueprint to make more copies of the virus. The RNA is surrounded by a lipid (fat) membrane.
2. Within that membrane are a number of proteins. The spike protein (S-protein) is like a hook that allows it to attach to cells of the host that it invades. Once the virus has attached to a host cell, the envelope protein (E-protein) of the virus triggers the host cell to start replicating the viral RNA.
3. The S-protein of the SARS virus attaches to a particular part of the host cell membrane called the ACE2 receptor. The ACE2 receptor is like the doorway that lets SARS into your cells.
4. If you are taking certain classes of drugs for hypertension (ACE Inhibitors and ARBs) you will have more ACE2 receptors on your cells or the receptors are upregulated which means they are more active. To use my analogy, if you are on those type of drugs you have more doors to let SARS in and/or those doors are easier to open.
5. SARS CoV2 most commonly attaches to the ACE2 receptors in the cells lining your lungs. In particular, cells called Alveolar Type II (ATII) cells. The alveoli are the little air sacks that make up the lungs.
6. The cells that line these air sacks are the cells that let oxygen into your blood and let carbon dioxide out. The cells that perform this function are called the Alveolar Type I (ATI) cells. The ATII cells are responsible for producing fluid in the lungs (known as surfactant) which lines the alveoli walls facilitating the gas exchange.
7. When the SARS virus invades an ATII cell, the host body responds using its immune system.
8. Cells of your innate immune system (there are three levels to the immune system – physiological barrier, innate immune system and adaptive immune system) respond to the invasion of the host cells.
9. The cells of the innate immune system (macrophages and neutrophils) destroy the invaded host cells by a process of phagocytosis whereby infected cells are engulfed and broken down by enzyme activity within the macrophage. The fragments left by this process are known as antigens.
10. As more ATII cells become infected, less surfactant is produced in the lungs. This leads to the ‘dry cough’ symptom. If the number of damaged ATII cells becomes large, then the alveolar cells (ATI cells) that carry out the gas exchange in the lungs, collapse. This leads to low oxygen levels in the patient.
11. The triggered macrophages and neutrophils release proteins known as cytokines.
12. Cytokines are proteins that regulate the body’s immune system and inflammatory response. The three key players in the response to COVID-19 infection are TNF-α, IL-1 and IL-6 but there are many more. Some are pro-inflammatory; some are anti-inflammatory.
13. As the level of infection increases, and the macrophage activity increases, the level of these cytokines increases.
14. Cytokines can pass through the blood brain barrier. In the brain they signal to the hypothalamus to up-regulate body temperature, leading to the fever that is symptomatic of COVID-19 infection.
15. Higher levels of cytokines leads to many responses: Blood vessel walls become more prone to effusion, which allows blood to pass out of the blood vessel and infiltrate the surrounding tissue. This is an important part of the response as it allows the macrophages which are transported in the blood to reach the invaded cells. But, if the cytokine level is too strong, too much blood leaves the vessels, leading to the shock response and decreased blood flow to the organs in extremum, leading to organ failure.
16. The macrophages and neutrophils in type 2 diabetics and those with excess adiposity (fat storage) have decreased ability to perform phagocytosis (the ability to engulf and destroy the infected cells).
17. Type 2 diabetics and those with excess adiposity have increased baseline levels of these cytokines, particularly those that stimulate inflammation – paraphrasing, they have more inflammatory cytokines already in circulation. They are therefore more likely to have an enhanced cytokine response to infection: Excess fever, excess blood effusion and excess inflammation are more likely to occur in these patients.
18. Above a certain threshold of infection, these patients are more likely to enter an out of control cytokine response – more cytokines, more inflammatory response, more cell damage, more cytokines. This has been labelled the ‘cytokine storm’ in the media.
19. Viral vaccines work by deactivating (usually) the S-protein or E-protein of a virus, thereby preventing it from attaching to host cells or, if it does attach, stopping it from taking over the host cell machinery.
20. If a virus mutates the shape of the S-protein or E-protein might change.
21. A vaccine that works for one shape of these proteins may not work against the mutated forms of the proteins. A vaccine might therefore be specific to one or a subset of the viral strains if there are many mutated variants in the population.
22. The adaptive immune system in the human body is the system that produces our own natural immunity via antibodies to the invading pathogen. During the initial infection, the cells of the adaptive immune system are triggered to destroy fragments of the invaded host cells not removed by the innate immune system. Specifically they produce antibodies to the fragments of the virus not destroyed by the innate immune system. These remaining fragments are known as antigens.
23. Once the infection has been resolved, the adaptive immune system keeps some of the cells (known as memory cells) which can be recruited quickly should the same antigens reappear in a re-infection.
24. We are not yet sure how robustly natural immunity to SARS will protect against future infection.