Posted 14 May 2020
An interesting bit of geekery today.
Here in the UK we make much of the ‘excess deaths’ figures, that is, how many people have died over and above a normal or ‘average’ year. Currently this stands at over 50,000.
Some of the excess deaths are directly attributed to coronavirus – COVID19 is identified at the registration of those deaths. But not for all of the excess deaths.
‘The gap’, is the total number of excess deaths minus the COVID19 registered deaths. There are a lot of competing explanations for ‘the gap’.
At one extreme, we could just assume all ‘gap’ deaths should have been COVID19 deaths, it is just that at the death registration this was not tested-for or determined. We could then move away from that extreme and say some of those gap deaths are due to illnesses, or lack of treatment of illness, caused directly or indirectly by the measures taken to combat COVID19. Worsening of chronic illness, social isolation, depression could all be contributory. No one at this stage knows for sure how this latter group of causes contribute to the gap.
Understanding the gap is pretty important though. If we have a better estimate of true deaths and also, separately, have a better idea how many of us in total have had the infection but recovered, we get more accurate estimates of the parameters that contribute to the 1-5 monitoring system. Knowing how many of us have yet to be infected and if we do get infected, what are the true risks of us dying are pivotal metrics to future action.
I read a great paper today from the U.S. (regrettably I am not sure how much of the result translates to the U.K. but it is interesting nonetheless) where researchers have been very resourceful at looking for what data are available even if at first it might not seem promising as a source of information.
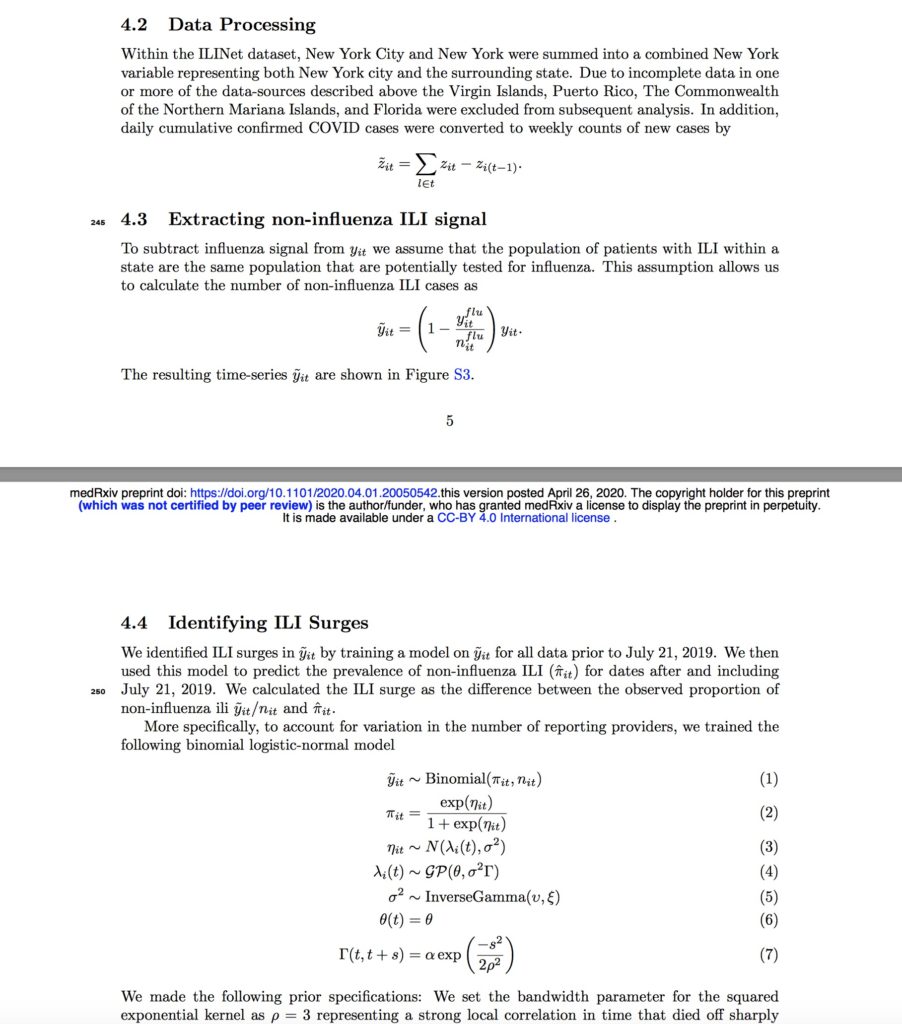
It seems that in the US, they have something called the ‘ILI outpatient surveillance data’ service. ILI is ‘Influenza Like Infection’. Across all 50 states they have a recording system for people who enter the medical care services with influenza like symptoms but then through testing, are determined not to have influenza as the causative pathogen. The symptoms that determine ‘ILI’ are pretty much the same symptoms that are shown by mildly symptomatic COVID19 cases, or symptoms that mark the early stages of a more severe COVID19 course. And there is the clever linking.
The beauty of the ILI system is that it has been running for quite a number of years, so there are long term data on what the non-influenza ILI cases should be in an ‘average’ year. Of course in March 2020 there are a lot more than in an average year and I could call these ‘excess ILI cases’ (by a normal March ILI cases are normally subsiding as the flu season is ending). Of course, there are more excess ILI cases than there are test-positive COVID19 cases. So there is ‘a gap’: Excess ILI cases minus COVID19 positive cases. Sound familiar? Excess and gap? Of course, this is interesting as it gives possible information about cases; the excess and gap in the UK data are in the deaths data.
I will spare you detail: The maths is both elegant yet scary (I copy some of the equations and graphs to show you why my head now hurts). But the model results are interesting (…but remember my moto from a few days ago: All models are wrong, some are useful). Anyway the outcome of all the modelling in this case is that from 8-28 March, in the 50 U.S. states ‘official’ new COVID19 case numbers could have been under-estimating true case numbers by 8.7 million in that three week period alone. The reported cases in that period were 105,000. These means only 1.2% of all cases were captured.
The model also shows case-doubling every 4-5 days (how long it takes for 10 cases to become 20, 20 to become 40 and so on). If this is true and the first cases were in January, then a significant proportion of the population must have been exposed. (That is just expressing the same data result in another way).
This is of course a staggering discrepancy, but we have the same problem as the UK excess and gap data: Finding robust mechanisms to account for these discrepancies. Non influenza ILI cases were very significantly up and no other known pathogen is thought to be have a surge on the back of coronavirus. Equally, the excess, ILI cannot be purely psychosomatic as the tests for ILI include objective tests when presenting into a medical facility. Inevitably though in a time of pandemic, the power of the mind in the patients will be strong. Lots of things to ponder.
The paper quite rightly expresses the findings as inputs for further study, but nonetheless it is intriguing.
